








Ischaemic heart diseases (IHD) – mainly MI – represent a large disease burden all over the world. Almost 18 million people die each year from cardiovascular diseases, accounting for 31 % of deaths globally.1 Ticagrelor, the more potent cousin of antiplatelet therapy clopidogrel, has been shown to reduce the composite endpoint of death from vascular causes, MI or stroke by an additional 16 % compared with clopidogrel when used with aspirin.2 Controversially, a meta-analysis of similar patient groups in Asia demonstrated that these ticagrelor benefits did not seem to be replicated in Asians, and Asian patients treated with ticagrelor experienced more bleeding. Even less is known about a third P2Y12 inhibitor, prasugrel.3,4
While international guidelines promote the use of ticagrelor and prasugrel over clopidogrel for patients with acute coronary syndrome (ACS) after percutaneous coronary intervention (PCI), the World Heart Federation issued a consensus statement in 2014 on antiplatelet use in East Asians with ACS or requiring PCI, clearly stating that there is insufficient data to suggest that ticagrelor or prasugrel are superior to clopidogrel for this patient group.5 Notably, East Asian patients have a similar or an even lower rate of ischaemic events after PCI compared with Caucasian patients, despite a higher level of platelet reactivity during dual antiplatelet therapy (DAPT). Asians have also been found to have a higher risk of bleeding. This has been dubbed the ‘East Asian Paradox’, and it has been suggested that there should be a different approaches to treatment for Caucasian patients and Asian patients who have undergone PCI.5,6
The clinical benefits of ticagrelor and prasugrel come at a price – not only do they cost more than clopidogrel, but they also increase the risk of bleeding. In the Trial to Assess Improvement in Therapeutic Outcomes by Optimizing Platelet Inhibition with Prasugrel–Thrombolysis in Myocardial Infarction (TRITON TIMI) 38, the medical community was warned about the use of prasugrel in patients with a past history of stroke, age >75 years and a body weight <60 kg.7 Consequently in Japan, the dose labelled for use was one-third of the dose used in Caucasians.8
Additionally, the Asian counterpart, Phase the International Study of Ticagrelor and Clinical Outcomes in Asian ACS Patients (PHILO) study, was not able to replicate the ischaemic benefits seen in US patients in the PLATelet Inhibition and Patient Outcomes (PLATO) trial; and the bleeding rate was twice that seen in PLATO.2,9 In the Prevention of Cardiovascular Events in Patients with Prior Heart Attack Using Ticagrelor Compared to Placebo on a Background of Aspirin (PEGASUS) trial, ticagrelor was used for an extended period at a reduced dose of 60 mg twice daily beyond the first year, and the number needed to treat (NNT) and number needed to harm (NNH) was similar at three years (79 versus 81, respectively).10
More recently, there have been a series of guided strategies for de-escalation of antiplatelet therapy.11 The strategy to de-escalate could be driven by the risk of bleeding (unguided), or platelet reactivity testing (guided). This could be particularly important for Asians, as illustrated in a large registry study of patients with ST-elevation MI (STEMI) that identified Asian ethnicity as an independent predictor of major in-hospital bleeding compared with Caucasians (3.6 % versus 2.2 %, p<0.001; OR 1.32, p<0.001).12
In our single-centre observational study of 349 Asian STEMI subjects started on ticagrelor, there were 8.5 % clinically significant bleeds for those receiving ticagrelor for a full 12 months duration, compared with 7.8 % in the de-escalated group (HR 3.36; p=0.047). In the de-escalated group, 5.9 % of bleeds occurred while on ticagrelor and only 1.8 % while on clopidogrel (unpublished data). Notably, the net clinical benefit study Timing of Platelet Inhibition After Acute Coronary syndrome (TOPIC) demonstrated that the strategy of unguided de-escalation of ticagrelor to clopidogrel at 1 month does not result in increased risk of ischaemic events but significantly reduces bleeding at 1 year.13 Its platelet function sub-study TOPIC Vasodilator-Stimulated Phosphoprotein (TOPIC-VASP) elucidated that while de-escalation was superior regardless of initial platelet reactivity, the benefit was greater in low on-treatment platelet reactivity patients.14 The European Society of Cardiology 2018 guidelines for myocardial revascularisation now alludes to the potential use of platelet reactivity testing to consider de-escalation of antiplatelet therapy.15
CYP2C19 genotype mutations and its associations with greater major adverse cardiovascular event (MACE) risk is well documented. Numerous meta-analyses have demonstrated that CYP2C19 loss-of-function (LoF) alleles is associated with significantly worse ischaemic outcomes if clopidogrel is used in ACS patients undergoing PCI. While it is known that CYP2C19 genotype variations influence the antiplatelet activity of clopidogrel, neither ticagrelor nor prasugrel appear to be affected by the same mutations. This has led to international drug label approval bodies to acknowledge of the clinical significance of poor metaboliser (PM) and intermediate metaboliser (IM) phenotypes compared with extensive metaboliser (EM) and ultrarapid metaboliser (UM) phenotype groups, following the Clinical Pharmacogenetics Implementation Consortium guidelines.16 The American and Dutch guidelines recommend that ticagrelor or prasugrel should be used for PM and IM.16,17 Sorich’s meta-analysis revealed that Asian populations who had PCI and at least one LoF allele have worse ischaemic outcomes than with Caucasians with at least one LoF allele and PCI. The authors state that this is particularly worrying since the incidence of at least one LoF allele in Asians is 53.9 %, compared with 28.4 % in Caucasian patients.18
Our local data corroborates these authors’ findings, with LoF alleles present in at least 60 % of subjects studied.19,20 Furthermore, our own CLOpidogrel – PRAsugrel Switch study (CLOPRA) population comprising 247 patients with ACS found that those with PM are at 10-fold increased risk of developing an ischaemic event compared with those with EM (30.8 % versus 13.7 %, OR 10.2, p=0.042).16 Cohort studies based in America have shown that using alternatives to clopidogrel is associated with reduced ischaemic outcomes, while high dose clopidogrel did not seem to mitigate ischaemic risk of LoF subjects.21–23 The ongoing prospective randomised controlled trial, Tailored Antiplatelet Therapy Following PCI (TAILOR-PCI) which assigns LoF subjects to alternative treatments to clopidogrel, will give us firmer answers in regard to the effectiveness of alternatives in this group.24
How is platelet reactivity related to genotype mutation? An East Asian group undertook a prospective registry study comprising more than 4,000 subjects, looking at the genetic effects on platelet reactivity and 1-year outcomes. CYP2C19 was significantly associated with high on-treatment platelet reactivity (OPR), and the number of CYP2C19*R (*2 or *3) alleles was proportional to the increased risk of high OPR. The other single-nucleotide polymorphisms – CYP2C9, ABCB1, PON1 and P2Y12 – were not significantly associated with high OPR.25
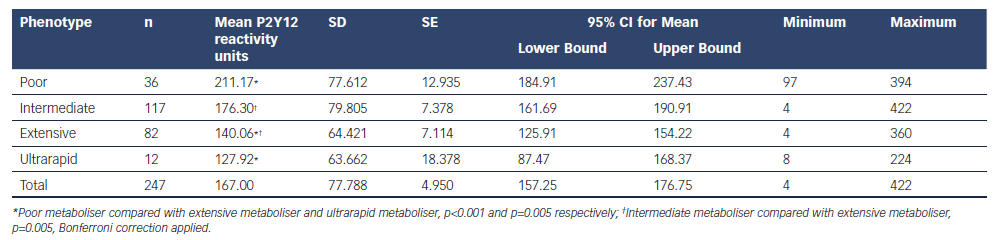
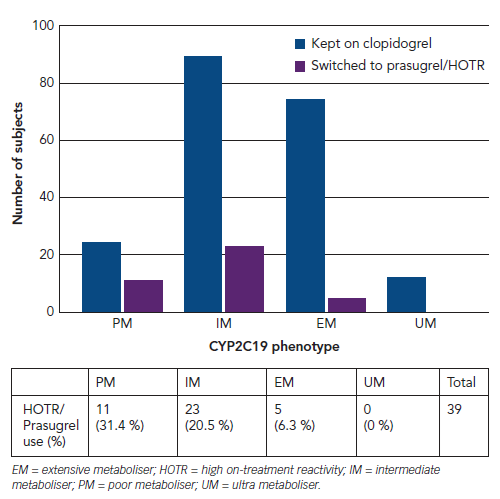
We present a similar relationship with our Southeast Asian CLOPRA subjects. Table 1 shows that the average OPR significantly differed when comparing PM with EM and UM (p<0.001 and p=0.005, respectively) and IM compared with EM (p=0.005). However, we also found that platelet reactivity testing, with P2Y12 reactivity units (PRU) cut-off at 230 only picked up 31.4 % and 20.5 % of PM and IM as high OPR (Figure 1). As PRU was used as the strategy to switch therapies, the majority of patients with IM and PM were kept on clopidogrel.
We thus had the opportunity to observe MACE and bleeding rates for the patients who were left on clopidogrel for the full duration of follow-up. We observed that the non-LoF clopidogrel patients experienced 1.1 % incidence of MACE while the event rate of LoF patients taking clopidogrel and LoF who were prescribed prasugrel were 8.8 % and 5.9 % respectively. LoF subjects who stayed on clopidogrel had a statistically significant 8.7-fold increased risk of MACE compared with non-LoF left on clopidogrel (p=0.041).
The clinical community has now been thrown into a conundrum in respect to how best to decide which P2Y12 inhibitor to use, for what duration, and if we should be using platelet reactivity, CYP2C19 phenotype or both to guide our choice of antiplatelet therapy. The most attractive, logical solution would be to use both platelet reactivity testing and CYP2C19 phenotype in decision-making algorithms, alongside traditional cardiovascular risk factors.26 Since the high OPR cut-off in Asians was suggested to be higher than that in Caucasian people, coupled with our findings, CYP2C19 genotype testing might be the more effective test to use.25 However, it is attractive to consider the use of rapid point-of-care platelet reactivity testing for two reasons: it offers the pharmacodynamics of how the antiplatelet is working, akin to how we use international normalised ratio for warfarin, and genotyping may take up to 3 days to run and discharge decisions have to be rapid, especially for escalation strategies. While we patiently await TAILOR-PCI findings based predominantly in countries with a mainly Caucasian population, now would be a great time to carry out large-scale, well-designed studies using either one or both gene and platelet reactivity assays to determine the best means to use both for an Asian population , especially in a real-world setting. However, platelet reactivity cut-offs must first be defined for Asians. For this to succeed, research, governmental and administration bodies and pharmaceutical industries must support the need for such large-scale, Asian studies. For now, it is certainly permissible to use pharmacogenomic testing to escalate antiplatelet therapy, and potentially de-escalate antiplatelet therapy in patients who have a high risk of bleeding.
Lastly, since Asian ethnicity is independently associated with major bleeding with ticagrelor and prasugrel, coupled with a higher incidence of CYP2C19 LOF, studying this issue is more pressing for Asians than for Caucasians.3,6 Biomarkers such as gene testing and platelet reactivity testing assist us in the holistic assessment of the risks of therapy and treatment. Therefore, there is certainly a strong case for routine gene testing for escalation or de-escalation, particularly in Asians, after there has been a holistic consideration of procedural or anatomical risk factors for MACE and factors associated with bleeding.20