







The term cardiac remodelling (REM) is used to define changes that produce geometrical rearrangement of the normal structures of the heart, together with complex biological and molecular alterations. REM affects the heart at the level of the cardiomyocyte, the blood vessels and the extracellular matrix. Proliferation of the latter, resulting in fibrosis, is one of the hallmarks of pathological REM.1,2 REM represents a major cause of heart failure as well as cardiac morbidity and mortality.
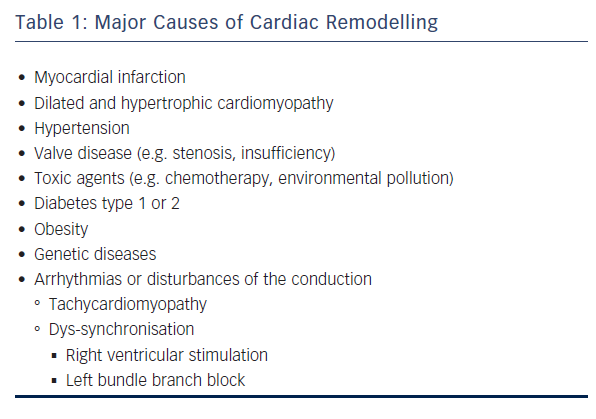
REM can be considered a universal phenomenon (see Table 1). It is initially considered an adaptive and physiological process but soon becomes maladaptive and pathological.2 REM can be the result of hypertension; cardiomyopathies, either dilated or ‘burnt-out’ hypertrophic obstructive cardiomyopathy; valvulopathies, especially those causing volume overload; antineoplastic drugs such as doxorubicin; diabetes; and senescence of cardiac fibroblasts.2
Arrhythmias are also associated with REM. The term tachycardiomyopathy was introduced approximately 30 years ago, to describe the impairment in left ventricular (LV) function secondary to chronic tachycardia. Tachycardiomyopathy is partially or completely reversible after normalisation of the heart rate. The condition is primarily caused by atrial fibrillation or flutter, atrioventricular tachycardia, atrioventricular nodal tachycardia and other arrhythmias characterised by tachycardia, including multiple premature ventricular contractions.3 Left bundle branch block (LBBB) can also unfavourably affect the myocardium through paradoxical septal motion. This observation has led to the application of arrhythmia ablation or cardiac resynchronisation therapy in REM.
However, the most common cause of REM is anterior acute myocardial infarction (AMI). Despite the use of primary percutaneous coronary intervention (PPCI) and optimal standard pharmacotherapy, REM ultimately occurs in 30 % of anterior AMIs. Non-anterior infarcts involve a smaller myocardial mass, thus REM occurs in only approximately 17 % of cases.4 The most well-understood mechanism underlying REM is infarct expansion, which is affected by wall stress.5
There is a need for a precise definition of REM. The historical definition of a 20 % increase of the left ventricular end-diastolic volume (LVEDV), first employed in 1986,6 is still in use today, although the left ventricular end-systolic volume (LVESV) and the LV mass have also been used as clinical endpoints.7 In the Global Utlilization of Streptokinase and Tissue Plasminogen Activator for Occluded Coronary Arteries (GUSTO 1) trial, LVESV was a strong prognostic indicator for early and late mortality.8 In a meta-analysis of 30 mortality trials of 25 drug/device therapies, Kramer et al.9 found that left ventricular ejection fraction (LVEF), LVEDV or LVESV were strongly associated with mortality. However, in studies to date, cut-off values have been arbitrary; continuous measurements are more meaningful. Farah et al.10 used a definition of REM of an increase of 10 % in ventricular endsystolic or end-diastolic diameter, and found a higher (58 %) incidence of REM after an anterior myocardial infarction (MI) compared with other studies. This highlights the need for consensus upon a common definition. In the Acute Myocardial Infarction Contrast Imaging (AMICI) trial, the term ’reverse REM’ was employed to denote a >10 % reduction in LVESV. In this study, Funaro et al.11 found a reverse REM at 6 months in 39 % of patients following PPCI. Reverse REM was the only independent predictor of 2-year event-free survival. In the Resynchronization Reverses Remodeling in Systolic Left Ventricular Dysfunction (REVERSE) study, Gold et al.12 used a definition of reverse REM of >15 % decrease in LVESV, and found that reverse REM improves prognosis. In routine clinical practice, many clinicians utilise ventricular dimension rather than volume. The definition of REM is also crucial for cardiovascular MRI-derived calculations.
Pathophysiology
The initial stimulus for ventricular enlargement is myocardial stretch resulting from myocyte loss, rendering an area akinetic or dyskinetic. The remaining normal myocardium overfunctions to compensate for the decline in cardiac function. The ensuing increase in ventricular mass decreases myocardial wall stress according to the law of Laplace, while LV dilation contributes towards the preservation of stroke volume (Starling’s law). The region remote from the MI develops LV hypertrophy, which is initially physiological and adaptive. However, this rapidly becomes pathological and maladaptive.2 According to Frey et al.,13 REM after an AMI represents eccentric hypertrophy due to volume overload and is characterised by the addition of sarcomeres in series and cardiomyocyte elongation. The term physiological REM is used to describe adaptive myocardial growth due to normal demands such as exercise or pregnancy.13,14 Whether the ’athlete’s heart‘ can lead to pathological REM has been the subject of discussion, but most experts agree that it rarely leads to irreversible REM;15 hypertrophy and dilation promptly regress after ’detraining’. In a study by Schiros,16 19 marathon runners had REM as defined by a 35 % LVEDV index (LVEDVI) and 50 % LVESV index (LVESVI) increase, but also had a 34 % increased stroke volume index (SVI) and a normal ejection fraction (EF). In addition, their hearts remained elliptical while those of the comparison group of patients with mitral regurgitation (MR) become more spherical, a characteristic of REM.
Regarding molecular changes, the term ’subcellular remodelling’ has been employed by Dhalla et al.17 to include changes in the extracellular matrix, sarcolemma, sarcoplasmic reticulum, myofibrils, mitochondria, nucleus, as well as abnormalities in protein content, gene expression and enzyme activities. In terms of myocyte biology, the most important alteration is the activation of the foetal gene programme.1,2,17 This alteration in myosin gene expression involves the increase of the embryonic beta-myosin heavy chain (beta-MHC) and the decrease of alpha-myosin heavy chain (alpha-MHC). The latter is the minor component in humans (not more than 10 % versus >70 % in the rodent), but even a 2 % unit decrease can be associated with myocardial dysfunction. Beta-MCH has lower ATPase activity, which is associated with lower velocity of contraction. In addition, cardiac cells express a variant of Na+/K+-ATPase, which has poorer membrane stabilising capacity. Another major component of the foetal phenotype is the metabolic switch from fatty acid oxidation to glycolysis. This results into a net deficit of adenosine triphosphate (ATP) production and energy starvation.18
Other molecular changes include the decreased expression of many important genes, such as the sarcoplasmic reticulum Ca2+ ATPase 2 (SERCA-2), and the beta1 adrenergic receptors. In addition, the overexpression of natriuretic peptides and genes directing myocyte lengthening have been reported.1 In studies of rats, the thyroid hormone receptor alpha1 (TRalpha1) is downregulated, and an unfavourable balance among stress kinases has been observed.19 Thyroid hormones are responsible for increases in alpha-MHC, SERCA-2 and a decrease in apoptosis,20 while other changes may be attributed to inflammation. Many of these changes are interrelated – SERCA-2 itself is antiapoptotic; however, its level decreases with apoptosis. Thus a vicious circle emerges, centred around the infarct area. However, the area surrounding the infarct, the border zone, is also important.
The Border Zone
The concept of the border zone, an area between the infarct zone and the remote area, was introduced almost 35 years ago.21 Its enlargement in the early post-infarct days is considered responsible for the occurrence of infarct expansion, which is a key contributor to REM.5 The border zone has been shown to be a site of apoptosis for up to several months in animal studies and even longer in humans.22 If this area can be salvaged, cell death may be restricted; otherwise the akinetic or dyskinetic area expands and gradually affects the remote area.2 The border zone is also a site of reduced autophagy (a protective mechanism), activated inflammatory process and decreased SERCA-2 activity, and is a major target of therapeutic interventions. Interestingly, it is a preferential site for the engraftment of progenitor cells administered by the intracoronary route, but also the area in which native progenitor cells are expressed after an AMI, together with the activation of pro-regenerative and anti-apoptotic factors.23
Interaction of Processes with Therapeutic Implications
During an AMI, necrotic cardiomyocytes induce the production of reactive oxygen species (ROS), as well as the activation of inflammatory factors (toll-like receptors [TLRs], nuclear factor-kappaB [NF-kappaB]) and monocyte/macrophages. These processes are part of innate immunity.24 Replacement fibrosis is the end result of cell death1 and a hallmark of REM; this process is also induced by an increase of endocardial stress through mechanotransduction. Distefano et al.25 state that in REM numerous systems are dysregulated, primarily chronic contractile dysfunction, which is associated with neurohumoral activation. Other important pathways include the renin-angiotensin-aldosterone, endothelin, adrenergic and cytokine and growth factor systems. Therapeutic efforts should be directed towards the correction of these dysregulated processes. Burchfield et al.2 describe alterations in various arrhythmogenic processes, which manifest as ’electrophysiological REM’ with malignant ventricular arrhythmias.
Diagnosis
Since REM is primarily defined by LV dilation, echocardiography is the major diagnostic modality, and also has prognostic significance, since worse outcomes correlate with an increased end-systolic or end-diastolic volume. Increased sphericity is also a diagnostic criterion of REM.
MRI is increasingly being used in the diagnosis of REM. In addition to measurement of LV volumes, it gives important information about the presence and extent of fibrosis and absence of viability.
Traditional radioisotopic techniques provide indirect information regarding viability and as predictors of REM.26 Another emerging technique is in vivo imaging of molecular markers, some of which may have clinical application in the near future, such as those regulating collagen (metalloproteinases and their tissue inhibitors), vasculogenesis (integrins, vascular endothelial growth factor, smooth muscle actin) and those involved in growth and viability, including transforming growth factor-beta (TGF-beta), myofibroblasts and apoptotic markers. Many other markers, either radioisotopic or provided by MRI are also under clinical investigation.27
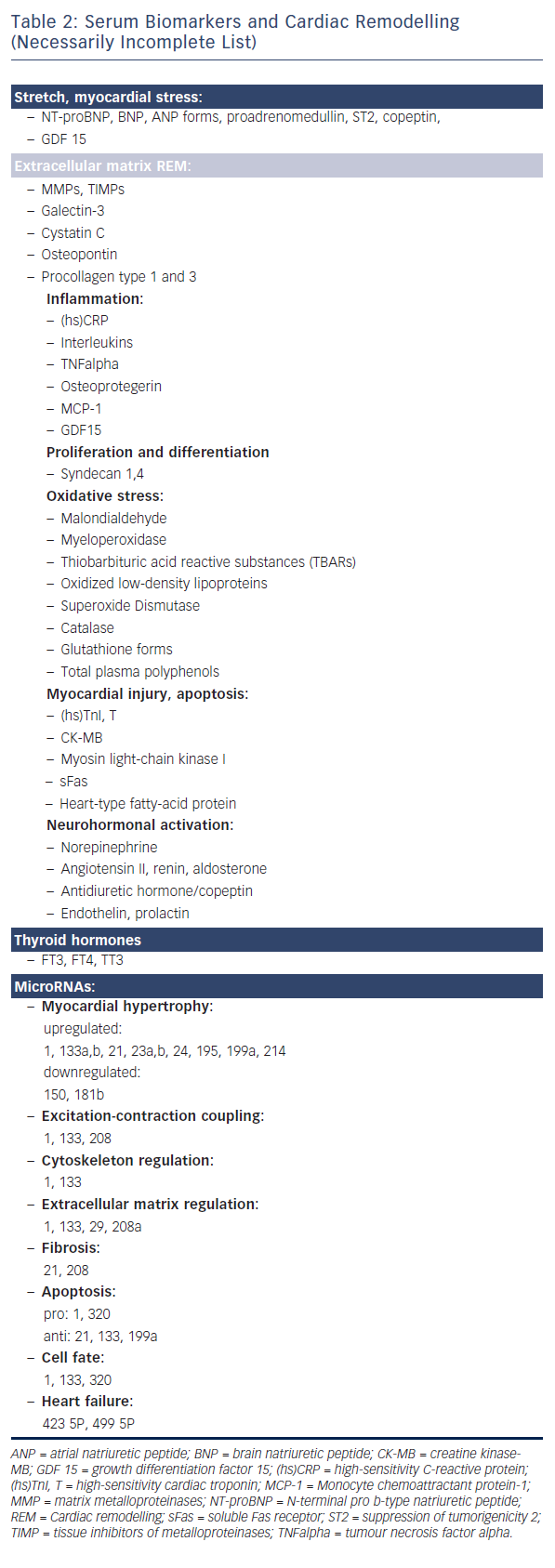
Numerous molecular processes are involved in the pathogenesis of REM. To date, these have only been studied in animal models. However, increasing numbers of biomarkers are being detected in the serum, as shown in Table 2. Many of these, such as N-terminal pro b-type natriuretic peptide (NT-proBNP) and suppression of tumorigenicity 2 (ST2), have not only diagnostic but also prognostic value. Most of these biomarkers represent the initial adaptive processes of REM. Thus the natriuretic peptides have vasodilator activities28 and growth differentiation factor 15 (GDF 15) is a regenerative factor.29 Syndecan is anti-apoptotic30 and ST2 is cardioprotective.31
MicroRNAs are potentially important biomarkers of REM.32 These ubiquitous non-coding RNA molecules (approximately 18–25 nucleotides in size) contribute in diverse ways to the pathogenetic mechanisms of REM, and may be reliable biomarkers because their plasma levels change in time-dependent mode after MI, particularly those that are relative to growth, fibrosis, angiogenesis and viability.
Therapeutic Approaches
Early Efforts
The main aim of early therapeutic approaches is to limit the size of the infarct. Death of ≥40 % of the LV myocardium is fatal; a diminution of MI size to 20 % of the left ventricle significantly improves prognosis. This may be achieved by:
- Revascularisation by PPCI as early as possible. In the absence of PPCI, early thrombolysis should be considered. Ndrepepa et al.33 studied 626 patients with first AMI who underwent PPCI. Patients with an anterior infarct and initially worse LV function had the greatest EF improvement at 6 months. Diabetics and smokers had a worse clinical course. Overall, 366/626 (58.4 %) improved while 130/626 (20.7 %) decreased their EF. Patients with decreased LV function had a worse prognosis at 3 years, (5.6 % mortality versus 1.2 % in those whose LV function improved).
- Adjunctive measures. Numerous approaches exist and are mostly directed towards mitigation of ischaemia/reperfusion injury, which accounts for up to 40–50 % of the total infarct size.34 A report from the European Society of Cardiology Working Group on Cellular Biology of the Heart35 listed 14 proven, 15 promising/uncertain and 17 negative drug studies and interventions, and concluded that most of these techniques did not reduce infarct size. Furthermore, the report concluded that there is currently no effective clinical therapy for protecting the heart against the detrimental effects of acute ischaemia/reperfusion injury.35 Adenosine and nicorandil have not gained wide clinical acceptance. However, new data on an old drug are interesting. The Effect of Metoprolol in Cardioprotection During an Acute Myocardial Infarction (METOCARD-CNIC) trial showed that metoprolol is effective when administered intravenously in conjunction with PPCI.36 Another proposed intervention is postconditioning, which comprises the application of brief periods of ischaemia early after reperfusion, and may be administered during PPCI. Most studies to date have involved remote postconditioning, which consists of 3–4 periods of inflating-deflating a sphygmomanometer in one or both arms and/or the thigh. Studies have shown that remote post-conditioning can induce reduction of infarct size in patients with ST-segment elevation MI.37
Long-term Therapy
Subsequent therapeutic approaches are administered immediately after PPCI. These include the ’big 4’, i.e. angiotensin-converting enzyme (ACE) inhibitors, or angiotensin receptor blockers (ARBs), beta-blockers, aldosterone antagonists and statins.38 ACE inhibitors, ARBs and beta-blockers have been successful in reducing heart failure morbidity and mortality following REM.39 In the Perindopril and Remodelling in Elderly with Acute Myocardial Infarction (PREAMI) study, the ACE inhibitor perindopril prevented the increase in LVEDV and also decreased REM by 45 % as compared with a placebo.40 In the large (n=6,405) Gruppo Italiano per lo Studio della Sopravvivenza nell’Infarto Miocardico: effects of lisinopril and transdermal glyceryl trinitrate, both singly and combined, on 6-week mortality and ventricular function after acute MI (GISSI-3) trial, lisinopril also decreased REM. Interestingly, REM occurred only in patients with a wall asynergy ≥27 %.41 In the Valsartan in Acute Myocardial Infarction (VALIANT) study, valsartan also proved effective in decreasing REM.42
Beta-blockers have been shown to exert anti-REM effects both in the experimental animal and in clinical studies.38,39,43 Hayashi et al. have shown that immediate administration of spironolactone prevents LV REM in patients with first anterior MI.44 However, the results of the recent Aldosterone Receptor Blockade in Diastolic Heart Failure (ALBATROSS) trial were disappointing – intravenous canrenoate followed by oral spironolactone for 6 months in patients with MI without heart failure (77 % ST-segment elevation myocardial infarction [STEMI], 23 % non-ST-segment elevation myocardial infarction [NSTEMI]) failed to decrease worsening heart failure, an indirect indication of REM.45 Statins have demonstrated antiinflammatory effects in animal models but have not proven effective against REM in clinical studies.46 However, Kjekshus47 suggests that by decreasing subsequent acute coronary events, producing new loss of cardiomyocytes, statins may prevent REM in the long term.
It should be noted that a large number of animal studies have demonstrated substantial reductions in REM. This highlights the differences between ‘mice and men’ – animal hearts are intrinsically normal, while the majority of patients suffering an AMI have widespread coronary artery disease that may adversely affect non-infarct areas. It has also been shown that myocardial areas subtended by a stenotic coronary artery cannot be preconditioned. Moreover, the majority of patients suffering AMI are taking multiple drugs, which may have important interactions. In addition, laboratory animals are genetically homogeneous, while humans have numerous polymorphisms (at least 50 have been proposed), which can affect infarct size and subsequently REM.47
Novel Drugs and Therapies
Some newly emerging drugs are non-toxic and can easily be administered for long periods of time.
Ivabradine. Apart from its heart rate lowering benefit, this drug has been shown to reduce apoptosis and REM in the Systolic Heart Failure Treatment with the I(f) Inhibitor Ivabradine Trial (SHIFT).7 Ivabradine is a useful alternative to useful al in patients who cannot tolerate the beta-blockers.48
Metabolic modulators. These can be divided in two subgroups:
- Insulinotropic and insulin-mimetic. To date, metformin is the most promising drug in this category.49 Exenatide and liraglutide have been successfully studied in animal models and would be easy to use in humans.
- Drugs affecting the shift from free fatty acids (FFA) to glucose oxidation. Trimetazidine has been successful in chronic congestive heart failure but has not been studied following AMI.50 It must be stressed that ’shifting’ energy production is difficult.
Another potentially important therapeutic target is chronic post-AMI ongoing ischaemia. This induces ROS production, Ca2+ dyshomeostasis and cell death. Ranolazine, a late Na+ inward channel inhibitor that is used in chronic angina pectoris, is currently being investigated.51
Tetracyclines are anti-apoptotic and promote SERCA-2 expression; doxycycline has proven beneficial in post-AMI patients with a low post-percutaneous coronary intervention (PCI) residual flow.52 Other agents under investigation include omega3 fatty acids and antioxidants. Allopurinol, a widely used xanthine oxidase inhibitor, has been shown to decrease experimental post-MI REM.53
In an initial study of a small number of patients, cyclosporine administered at the time of AMI was effective against REM.54 However, in the Cyclosporine to Improve Clinical Outcome in ST-elevation Myocardial Infarction Patients (CIRCUS) trial, at 1-year, outcomes in the 390 patients in the cyclosporine group did not differ from those of the 396 patients in the placebo group.55
Monoamine oxidase (MAO) inhibitors, while primarily neuroprotective, are also anti-apoptotic in the myocardium. Promising initial results have been reported with the use of rasagiline in the post-MI rat.56
Thyroid hormones increase alpha-MHC, SERCA-2 and decrease apoptosis; studies have shown that thyroid supplementation in the animal prevents or reverses REM.20,57,58 Around 30 % of patients with congestive heart failure have low triiodothyronine (T3) levels, constituting the ’low T3 syndrome’.59 The ongoing Thyroid Hormone Replacement Therapy in ST Elevation Myocardial Infarction (THiRST) study60 has shown promising initial results.
Exercise is successful in reducing REM both in the animal and human,61 and is beneficial in patients that have undergone left ventricular assist device (LVAD) placement.62
Another emerging concept is post-MI continuous remote conditioning, which is successful in the animal.63 Currently three large multicentre clinical trials are ongoing.
Interventions, Revascularisation Surgery, Left Ventricular Assist Devices
Revascularisation surgery has been investigated over many years. Its success is dependent upon the persistence and extent of viability, according to two clinical studies.64,65 In the study by Carluccio et al.65 the degree of reverse REM did not differ between patients who underwent percutaneous interventions or bypass surgery.
The AMICI study showed that PPCI produces long-term reverse REM in up to 39 % of patients, and is associated with a better 2-year eventfree survival rate.11
The concept of the utility of surgical restoration of REM is under discussion. According to the results of the Surgical Treatment for Ischaemic Heart Failure (STICH) trial, an additional benefit over revascularisation alone was seen only when the post-operative end-systolic volume index was 70 mL/m2 or less.66 In addition, with both coronary artery bypass grafting (CABG) and CABG plus volume reduction, a decrease of LVESVI >30 % at 4 months was seen in 26 % of patients with a baseline LVESVI <60 mL/m2, in 36 % in those with a baseline LVESVI 60–90 mL/m2 and in 45 % of those with a baseline LVESVI >90 mL/m2. Numerous techniques have been proposed for reducing the size of the left ventricle, some of which have entered clinical practice.67
LVADs are increasingly being employed, not only as a bridge to transplantation but also as a destination therapy. These devices induce effective reverse REM expressed by an important decrease in chamber size together with molecular changes that can be summarised as follows:68,69
- an increase of beta-adrenergic receptor density and reactivity toward adrenergic stimulation;
- an improvement in calcium handling (increase of Na+/Ca2+ exchanger and SERCA-2);
- an increase of insulin-like growth factor 1 (IGF-1);
- a decrease of atrial natriuretic peptide (ANP) and chromogranin A and a normalisation of the matrix metalloproteinases (MMP)/tissue inhibitors of metalloproteinases (TIMP) ratio;
- a decrease in tumour necrosis factor alpha (TNFalpha) in tissue and plasma; and
- a decrease of plasma epinephrine, norepinephrine, renin, angiotensin II and arginine vasopressin levels.
Hall et al.70 studied six paired human heart samples harvested at the time of LVAD implant and at the time of LVAD explant. Improvements in ventricular function were maintained over 3.8 years and were associated with a molecular ‘signature’ that correlated to the integrin pathway signalling.
Mann and Burkhoff71 differentiate between ’reverse remodelling’ and myocardial recovery; although these entities share many pathways, the former term does not represent normalisation of the pathological condition. They argue that following LVAD support only 5 % of dysregulated genes actually revert to normal. Moreover, although LV chamber geometry may normalise, the LV wall thickness/radius ratio and subsequent wall stress do not normalise.
Resynchronisation therapy can prevent and also reverse REM, mainly in patients with a QRS >150 msec, and more in dilated than in ischaemic cardiomyopathy. LV dimensions are a critical prognostic factor. If the LV diastole volume index exceeds 125 mL/m2 a superior response has been reported.72 In addition, a greater 5-year decrease in mortality was seen in patients with a >15 % decrease in LVESV index.12
Future Therapies
Novel drugs are continuously being sought. In addition to the remarkable clinical improvements attributed to LCZ696 in the Prospective Comparison of ARNI with ACEI to Determine Impact on Global Mortality and Morbidity in Heart Failure (PARADIGM-HF) trial,73 the findings of von Lueder et al.74 suggest that LCZ696 improves REM in animal models.75
MicroRNAs are being studied as biomarkers in all phases of MI. The inhibition of pro-REM members is currently under investigation.76
Gene transfer is an area of active clinical research. To date, SERCA-2 appears the most promising; the CUPID1 phase I/phase II trial (n=39) showed a continued benefit at 3 years of follow-up,77 with an 82 % decrease in cardiovascular events. However, results of the CUPID2 phase II trial (n=343)78 were disappointing – the use of SERCA-2, delivered by an adeno-associated virus serotype 1 vector, did not result in any improvement at a 17.5 months follow-up compared to the control group. The high cost of this therapy precludes continued research in a large number of patients. It is important to highlight the need for complete evaluation of the degree of viable/non-fibrotic myocardium before any novel therapy is contemplated. Progenitor cell efforts have been ongoing for the past 12 years.38,79 If administered early (within 5–10 days of AMI) they can produce a gain in EF of 5 units in large anterior infarcts. A large multicentre trial with a primary endpoint of 2-year mortality is ongoing. At present, endogenous progenitor cell regeneration is inadequate to compensate for cell loss; its pharmacological boosting is a novel concept.79
Summary: Future Directions
A holistic approach should be applied against post-MI REM that constitutes a main cause of morbidity and mortality from ischaemic heart disease. This should comprise early revascularisation, appropriate drugs (including neurohormonal antagonism), metabolism optimisation80 and possibly post-conditioning supplementation.
In the case of an anterior infarct radioisotopes, additional echocardiographic techniques, MRI and enlistment of new biomarkers may provide a better insight into the mechanisms of REM.
Judicious use of diagnostic and therapeutic modalities may prevent and/or reverse REM, and improve life quality and span. This is a worthwhile though arduous task. Recently, Gerber et al.81 reported that between 1990 and 2000 and from 2001 to 2010 the 5 years’ survival in post-MI patients with heart failure improved from 61 to 54 %; an encouraging finding.